| VIVO Pathophysiology | Other Endocrine Tissues and Hormones |
Renin-Angiotensin-Aldosterone System (RAAS)

The action hero of this endocrine system is a small 8 amino acide peptide called angiotensin II, but like many fictional action heros, it becomes a hero in several stops. A short and understated description of the importance of angiotensin II is that it a key regulator of blood volume and peripheral vascular resistance. Additionally, it acts in concert with aldosterone from the adrenal gland to normalize disturbances in electrolyte balance, particular sodium and potassium. One thing is certain: if you are in a serious car accident or perhaps a sword fight, and lose a lot of blood, you will want a your renin-angiotensin-aldosterone system in top shape.
It should be noted before proceeding that there are several differences among species in details of the RAAS system that are sometimes of physiologic and clinical significance.
Generation of Angiotensin II
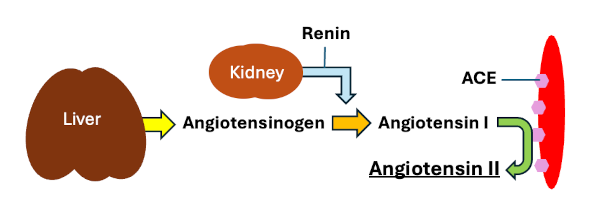
Angiotensin II is generated from a precursor molecule called angiotensinogen through a series of proteolytic cleavages. These cleavages can be summarized in the following sequence of events:
- Angiotensinogen is a large glycoprotein that is synthesized in the liver and secreted into blood.
- Circulating angiotensinogen is cleaved by the enzyme renin to release a 10-amino acid peptide called angiotensin I, which is still physiologically inactive. Renin is released from juxtaglomerular cells in the kidney when those cells sense low blood pressure (this is important - keep it in mind).
- Angiotensin I circulating in blood binds to a molecule appropriately called angiotensin-converting enzyme (ACE) and is cleaved to yield angiotensin II - the hero we've been waiting for all along. ACE is a membrane-bound enzyme that is embedded in the plasma membrane of vascular endothelial cells, most prominently in the lungs.
- Angiotensin II binds to one of two receptors designated AT1 and AT2 and those interactions promote the physiologic effects of this hormone. Binding to the AT1 receptor is the primary mechanism for the vasoconstrictive effects of angiotensin II.
Angiotensin II has numerous effects, but the best known and most clinically important of these is its ability to cause peripheral blood vessel constriction and thereby counter low blood pressure.
Now, where does aldosterone come into play in this story? Secretion of aldosterone from the adrenal glands is stimulated by two things: 1) high blood levels of potassium, and 2) angiotensin II. The major effects of aldosterone are to conserve water and sodium, and to promote excretion of potassum. Each of these effects is mediated by the effect of aldosterone on transport mechanisms in the tubules of the kidney.
Let's now put this all together and consider a situation in which you lose considerable blood (again, in an auto accident or sword fight). The following events rapidly unfold to save you:
- Following significant blood loss, blood volume and pressure drop leading to release of renin from the kidney.
- Renin cleaves circulating angiotensinogen to angiotensin I, which then is cleaved by ACE to generate angiotensin II.
- Angiotensin II does two things, both of which promote normalization of blood pressure:
- Contricts peripheral blood vessels to reduce vascular space and increase blood pressure.
- Stimulates aldosterone secretion, which helps minimize sodium and water excretion, again helping to maintain blood volume and pressure.
- You make it to the hospital and your injuries are hopefully repaired.
Inhibiting RAAS Activity
Although angiotensin II serves a vital role in protecting against such conditions as hypotension and blood loss, it can also contribute to a number of pathologic conditions, such as hypertension, congestive heart failure and some types of kidney disease. Hence, drugs that block the activity of RAAS are commonly prescribed in such conditions. The activity of RAAS can be suppressed in several ways.
ACE Inhibitors: Several drugs have been developed that inhibit angiotensin-converting enzyme or ACE and work by blocking the conversion of angiotensin I to angiotensin II. A few of many examples of widely used ACE inhibitors include benazepril, captopril, and enalapril.
Angiotensin II Receptor Blockers: These drugs prevent binding of angiotensin II to the AT1 receptor, thereby preventing this hormone-receptor interaction and subsequent physiologic response from occurring. Examples of these drugs include azilsartan, eprosartan, candesartan, irbesartan, losartan, telmisartan.
ACE inhibitors and AT1 receptor blockers are widely used for managing hypertension and other cardiac diseases. Although less commonly used, other approaches that are available include inhibitng renin release, which prevents conversion of angiotensinogen to angiotensin I, and inhibiting aldosterone activity.
Angiotensin-Converting Enzyme 2 (ACE2)
Many people are familiar with ACE2 due to its being the cellular receptor for SARS coronavirus-2 (SARS-CoV-2), the cause of the COVID19 pandemic. ACE2 is an enzyme distinct from ACE, but also is an important component of the RAAS. Like ACE, ACE2 is a peptidase, but unlike ACE, its major activity is to cleave the terminal amino acid off of angiotensin II to create what is called angiotensin (1-7) (7 amino acids). This seemingly small change has major consequences: angiotensin (1-7) has activities essentially the opposite of angiotensin II. The differences between these two forms of angiotensin are summarized as follows:
| Biologic Properties | ACE | ACE2 |
|---|---|---|
| Primary organ distribution | Lung | Heart, lung, kidney, intestine |
| Major Cellular Location | Lumenal (blood) side of vascular endothelial cells | Apical surface of epithelial cells (nasal and airway mucosa, intestinal epithelium |
| Peptidase activity | Removes 2 amino acids, converting angiotensin I to angiotensin II | Removes 1 amino acid, converting angiotensin II to angeiotensin (1-7) |
| Major effect on blood vessels | Vasoconstriction - increased blood pressure | Vasodilation - decreased blood pressure |
| Inhibited by standard ACE inhibitors | Yes | No |
| Receptor for SARS CoV-2 | No | Yes |
Updated March 2026. Send comments to Richard.Bowen@colostate.edu